The consistent and accurate documentation of patient progress is paramount to effective patient care and legal compliance within healthcare settings. A well-structured hospital progress note template provides a standardized framework for recording vital information, facilitating seamless communication between healthcare providers, and ensuring continuity of care. This article will delve into the essential components of a robust hospital progress note template, exploring its purpose, key features, and best practices for effective utilization. Hospital Progress Note Template is more than just a document; it’s a critical tool for optimizing patient outcomes and streamlining workflows. It’s a cornerstone of quality patient care and demonstrates a commitment to thorough record-keeping.
What is a Hospital Progress Note Template?
A hospital progress note template is a standardized document designed to systematically record a patient’s condition and response to treatment during a hospital stay. It’s a crucial component of patient care, providing a detailed account of the patient’s health status, interventions, and observations. Unlike a general medical record, a progress note focuses specifically on the patient’s experience within the hospital environment. It’s not just a chronological list of events; it’s a narrative that highlights the patient’s progress, challenges, and the care provided. The template’s purpose is to ensure that all healthcare providers involved have a clear and consistent understanding of the patient’s condition, enabling informed decision-making and coordinated care. Effective use of a progress note template significantly reduces errors, improves communication, and ultimately contributes to better patient outcomes.
Core Components of a Hospital Progress Note
A comprehensive hospital progress note typically includes several key sections. Each section is designed to capture specific information relevant to the patient’s care. Understanding these components is essential for creating accurate and useful notes. The following are some of the most frequently utilized sections:
1. Patient Demographics & Arrival Information
This initial section gathers essential patient information, ensuring a complete record of the patient’s arrival and initial assessment. It includes:
- Patient Name and Date of Birth
- Medical Record Number (MRN)
- Arrival Time and Location
- Reason for Admission (briefly stated)
- Attending Physician/Nurse Identifier
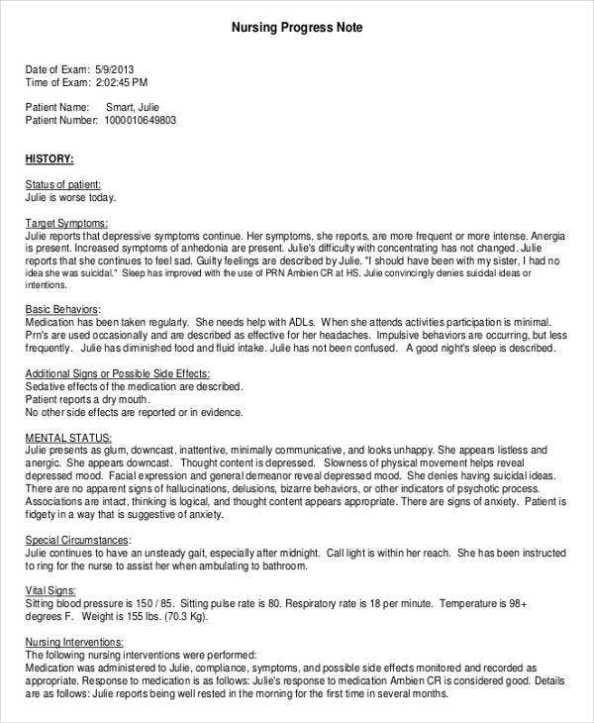
2. History of Present Illness (HPI)
The HPI is the cornerstone of the progress note. It describes the patient’s current condition, including the onset, duration, and characteristics of their symptoms. This section should be detailed and objective, focusing on what the patient reports rather than assumptions. Key elements include:
- Chief Complaint (the patient’s primary reason for seeking medical attention)
- Detailed Description of Symptoms (e.g., pain levels, shortness of breath, nausea)
- Relevant Past Medical History (e.g., previous surgeries, chronic conditions)
- Medications (current and past)
3. Physical Examination Findings
This section documents the results of the physical examination performed on the patient. It should include:
- Vital Signs (Temperature, Blood Pressure, Heart Rate, Respiratory Rate, Oxygen Saturation)
- Observations of Skin, Eyes, Ears, Nose, and Throat (O.E.T.)
- Assessment of Neurological Status (if applicable)
- Specific findings related to the patient’s condition
4. Diagnostic Tests & Investigations
This section details any diagnostic tests performed on the patient, including:
- Blood Tests (Complete Blood Count, Electrolytes, Liver Function Tests, etc.)
- Imaging Studies (X-rays, CT scans, MRIs)
- Other Tests (e.g., ECG, Urine Analysis)
5. Treatment Provided & Response
This is arguably the most critical section, outlining the interventions and treatments administered to the patient. It includes:
- Medications Administered (dosage, route, frequency)
- Procedures Performed (e.g., catheter insertion, wound dressing changes)
- Therapeutic Interventions (e.g., fluid administration, pain management)
- Patient Response to Treatment (e.g., improvement, worsening, stabilization)
6. Assessment & Plan
This section summarizes the patient’s current condition and outlines the plan for continued care. It should include:
- Current Diagnosis (if known)
- Prognosis (expected outcome)
- Further Investigations (if needed)
- Ongoing Treatment Plan (including medications, therapies, and follow-up appointments)
Utilizing the Hospital Progress Note Template Effectively
Creating a truly effective progress note requires careful attention to detail and a systematic approach. Here are some tips for maximizing the utility of the template:
- Be Objective: Focus on factual observations and avoid subjective interpretations.
- Use Clear and Concise Language: Avoid jargon and technical terms that the reader may not understand.
- Document Everything: Record all relevant information, even if it seems minor.
- Use Consistent Terminology: Employ the same terms consistently throughout the note.
- Include Relevant Images: Photographs of wounds, medications, or other relevant findings can be helpful.
- Maintain a Logical Flow: Organize the information in a clear and sequential manner.
The Importance of Documentation for Patient Safety
Proper hospital progress note documentation is not simply a bureaucratic requirement; it’s a critical element of patient safety. Accurate and complete records facilitate timely identification of potential complications, allow for effective communication among healthcare providers, and contribute to improved patient outcomes. Furthermore, well-documented records are essential for legal and regulatory compliance, protecting both patients and healthcare organizations. The ability to accurately track a patient’s progress and response to treatment is vital for ensuring continuity of care and promoting optimal patient well-being.
Conclusion
The hospital progress note template is a fundamental tool in modern healthcare. Its comprehensive nature, coupled with its ability to facilitate clear communication and detailed record-keeping, makes it an indispensable component of patient care. By understanding the core components, utilizing the template effectively, and prioritizing accurate documentation, healthcare professionals can significantly enhance patient safety and improve the quality of care delivered. Hospital Progress Note Template is a powerful instrument for optimizing patient outcomes and ensuring a safe and effective healthcare environment.
Conclusion
The consistent and accurate documentation of patient progress is paramount to effective patient care and legal compliance within healthcare settings. A well-structured hospital progress note template provides a standardized framework for recording vital information, facilitating seamless communication between healthcare providers, and ensuring continuity of care. It’s a critical component of quality patient care and demonstrates a commitment to thorough record-keeping. Effective use of a progress note template significantly reduces errors, improves communication, and ultimately contributes to better patient outcomes. The ability to accurately track a patient’s progress and response to treatment is vital for ensuring continuity of care and promoting optimal patient well-being. Hospital Progress Note Template is a powerful instrument for optimizing patient outcomes and ensuring a safe and effective healthcare environment.



